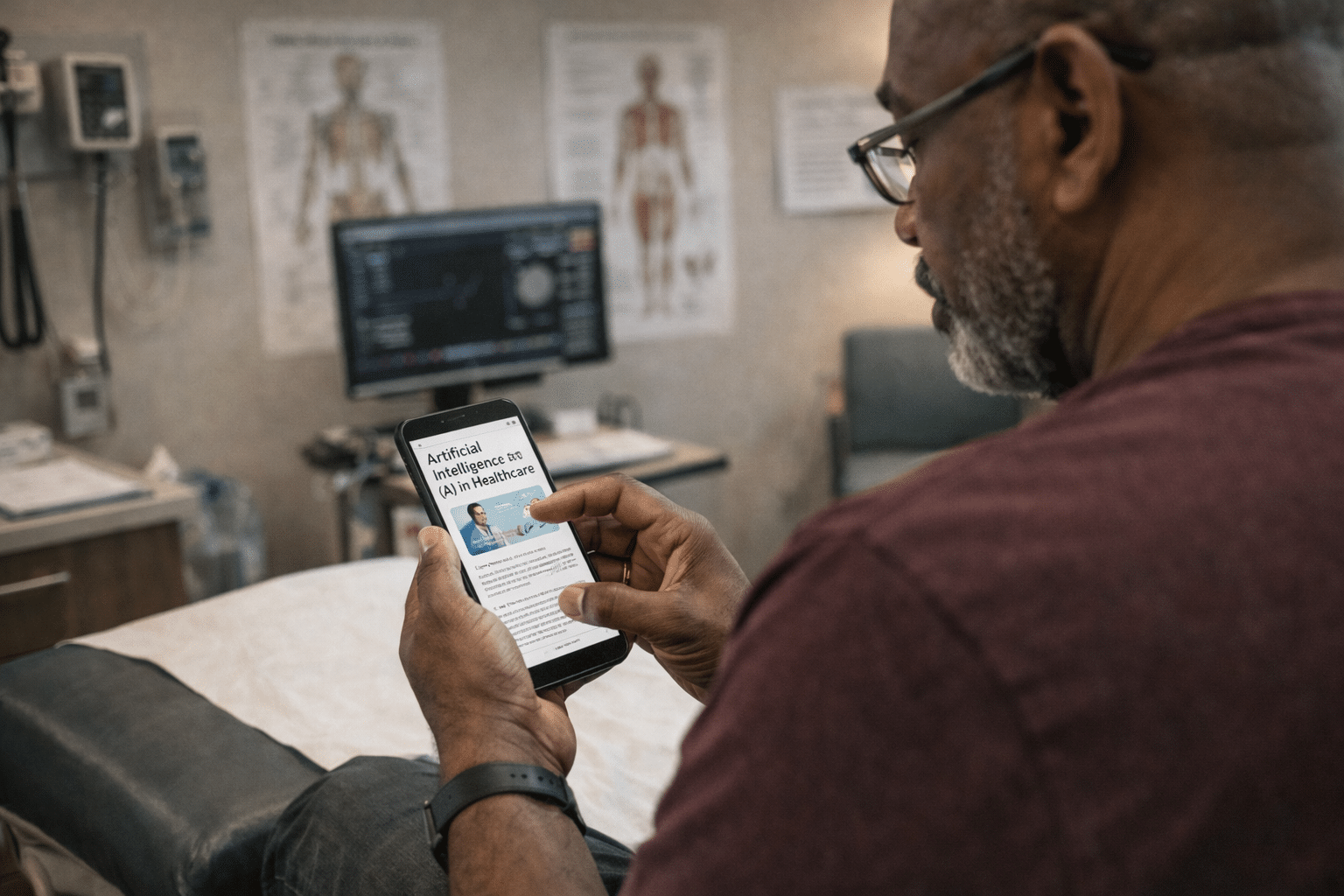
Artificial intelligence is no longer a futuristic concept in medicine. It is already in exam rooms, hospitals, insurance systems, and telehealth platforms. AI tools now help doctors draft clinical notes, flag high-risk patients, suggest diagnoses, predict hospital readmissions, and even recommend treatment plans.
In theory, these systems promise efficiency, earlier detection of illness, and better care coordination. But there’s a growing concern: if AI systems are trained on biased healthcare data — or built without transparency — they can amplify existing inequities rather than reduce them.
For Black patients in particular, this raises urgent questions. What happens when the same system that has historically under-treated pain, delayed diagnoses, and misjudged risk becomes digitized and automated? The answer is not simple. But it is serious.
RELATED: Is AI Rotting Your Brain?
When experts talk about “algorithmic bias,” it can sound abstract. In reality, bias in healthcare AI often looks like this:
These outcomes are not necessarily the result of malicious programming. Instead, they stem from how AI systems learn. AI models are trained on historical datasets — and those datasets reflect decades of unequal treatment, misdiagnosis, and systemic bias.
When past inequities are treated as neutral data, they become encoded into future decisions. That’s why bias in healthcare AI is not just a “tech problem.” It’s a healthcare equity problem.
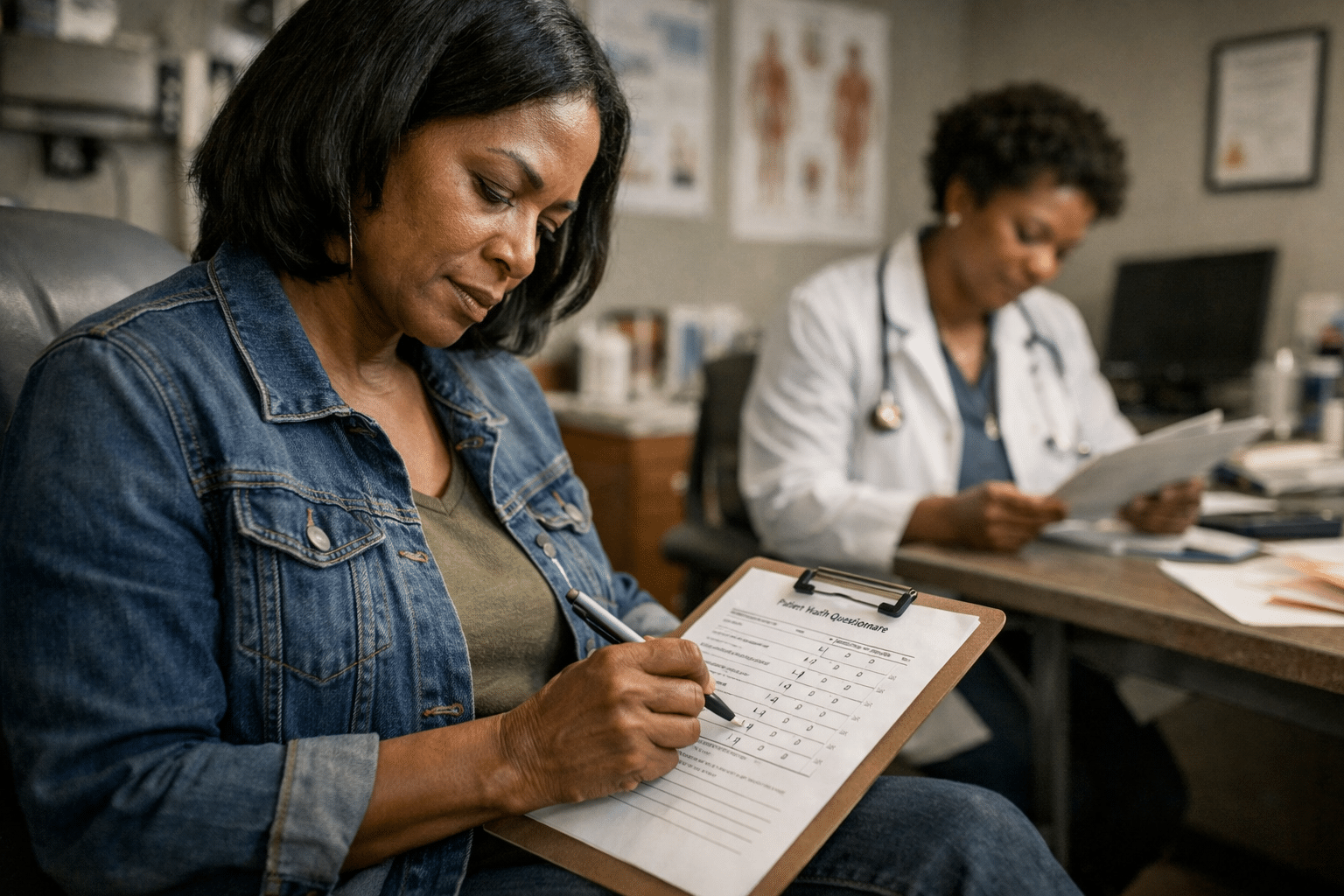
A recent study published in Cyberpsychology, Behavior, and Social Networking titled “The Augmented Exam Room: When AI Listens In—and Reshapes Trust” examines how AI tools integrated into clinical visits may reshape the doctor-patient relationship.
The study highlights concerns that:
When AI “listens in” to appointments — summarizing conversations or generating treatment suggestions — it changes the dynamic of care. If those tools carry hidden bias, the effects can ripple outward.
AI systems don’t understand fairness. They recognize patterns. If historical medical records show that Black patients received fewer diagnostic tests, the AI may learn that fewer tests are “normal.” If spending data shows less investment in Black patients’ care, the AI may interpret lower spending as lower need.
One widely cited case involved a healthcare algorithm that used healthcare costs as a proxy for illness severity. Because Black patients historically had less access to care — and therefore lower healthcare spending — the system ranked them as lower risk, even when they were equally sick.
This isn’t an isolated example. Research increasingly shows that large language models and predictive healthcare tools can reflect racial disparities present in training data. Bias becomes embedded not because AI intends harm — but because it mirrors the system that produced its data.
One of the most concerning aspects of healthcare AI is opacity. Many AI systems:
Without transparency, it is nearly impossible to detect whether an AI tool performs differently for different populations. For Black patients, this raises legitimate concerns:
Transparency is not just an ethical principle. It is a safety requirement.
If bias is not addressed, AI can worsen disparities in:
An AI-driven triage system might underestimate symptom severity in Black patients, delaying urgent care.
If predictive models recommend fewer interventions based on historical patterns, Black patients may continue receiving less aggressive treatment.
Language models used in patient-facing tools may generate stigmatizing or culturally insensitive guidance. The danger is scale. A biased human clinician affects dozens of patients. A biased AI system can affect millions. Automation accelerates impact.
It’s important to be clear: AI has the potential to improve access to healthcare, reduce administrative burden, and detect disease earlier. But technology is not neutral. It reflects the values and data that shape it. The goal is not to reject AI — it is to demand responsible design.
Patients have the right to ask:
Healthcare systems should not treat AI as invisible infrastructure. Patients deserve informed consent when automated systems influence their care.
Doctors and hospital systems should demand:
Clinicians should remain decision-makers — not passive recipients of algorithmic output.
Regulation has not kept pace with AI development. Policymakers should require:
Equity guardrails must be built into adoption — not added after harm occurs.
Healthcare AI can be transformative — but only if equity is treated as foundational, not optional. Responsible AI development includes:
Trust in healthcare is fragile. For Black communities, historical mistreatment has already eroded confidence in medical institutions. If AI systems reproduce inequity, that trust may fracture further.
Technology should not widen gaps. It should help close them. AI is already reshaping the exam room. It drafts notes, flags risks, and influences decisions — sometimes invisibly. But when healthcare AI is trained on biased data, it can perpetuate the very disparities medicine claims to address.
Bias in healthcare AI is not just a software flaw. It is a reflection of systemic inequality embedded in data. And without transparency, auditing, and accountability, those inequities can scale rapidly. Patients deserve clarity. Clinicians deserve tools they can trust. And policymakers must ensure that innovation does not outpace equity.
The future of AI in healthcare will not be defined by how advanced it becomes — but by how fair.

By subscribing, you consent to receive emails from BlackDoctor.com. You may unsubscribe at any time. Privacy Policy & Terms of Service.